



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 164 |
| Age: | 74 |
| Clinical presentation: | Postmenopausal woman with increased risk of breast cancer presented with right supraclavicular node she had first noticed 1 month ago. Since then it had increased in size. She had undergone right breast-conserving surgery for breast cancer 6 years earlier. On examination, a hard, non-tender supraclavicular lump was palpable in the right breast. A surgical scar in the right breast was seen with a palpable, diffuse, firm to hard area beneath the scar. The left breast was unremarkable. |
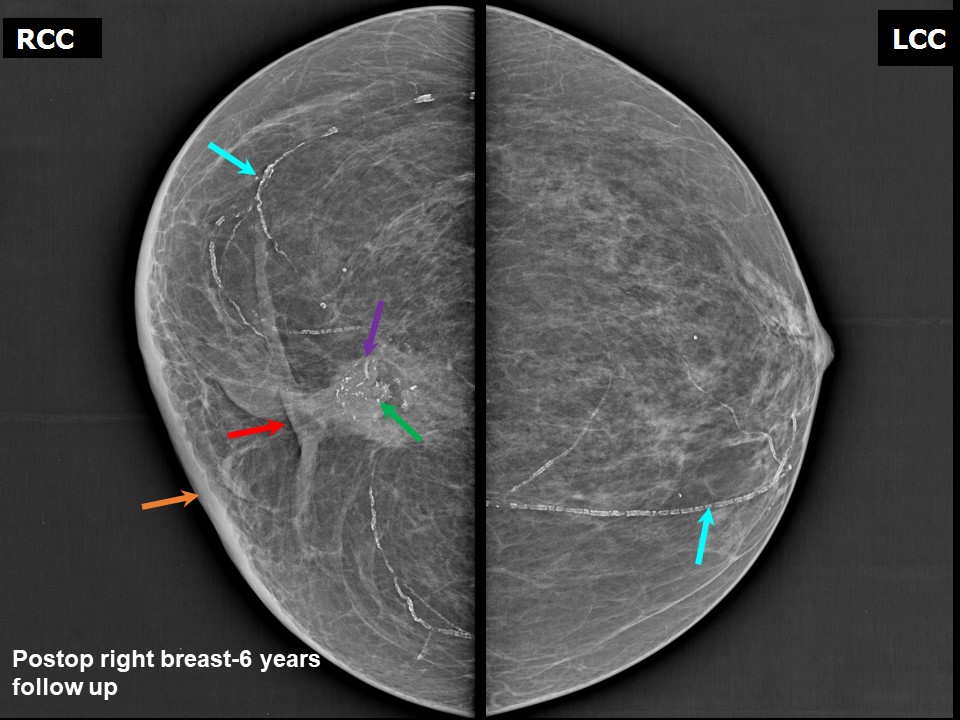
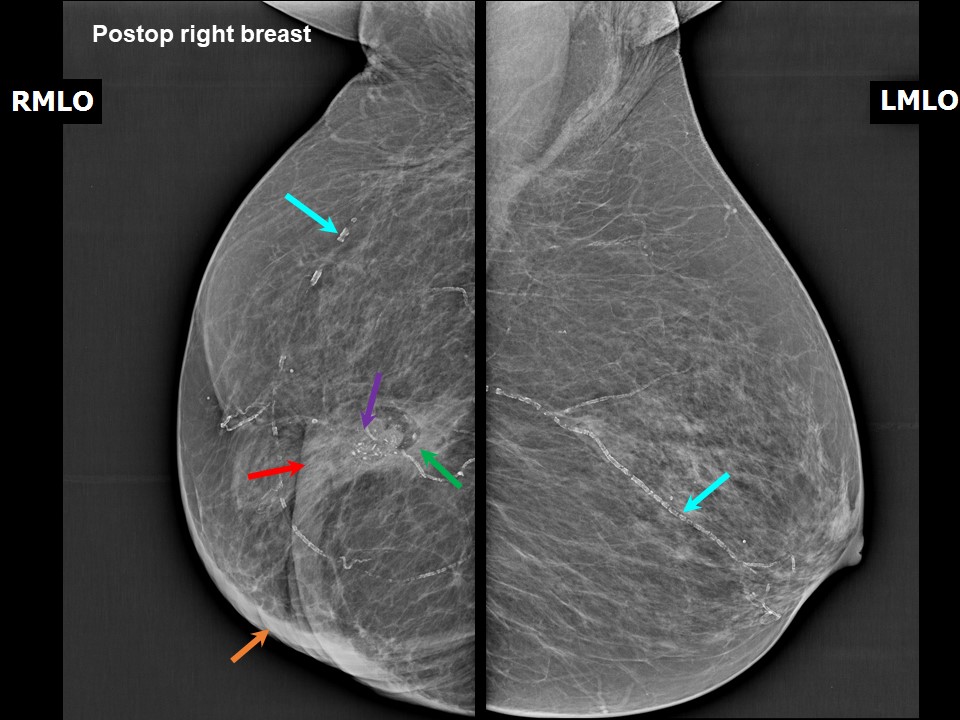
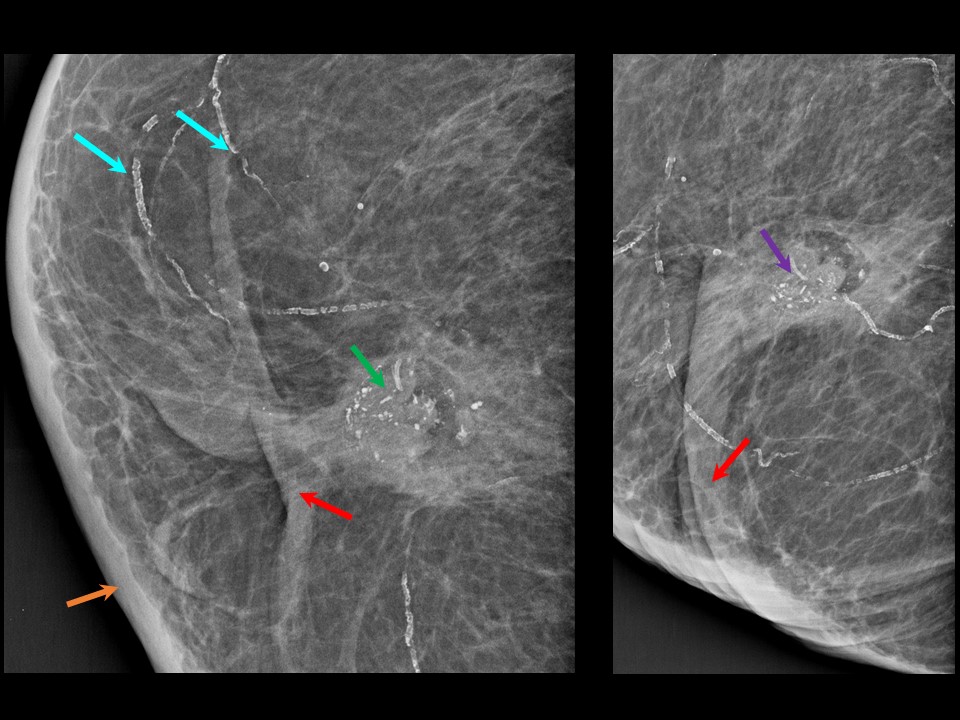
Mammography:
 |  |
 |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Postoperative right breast, upper inner quadrant at 1 o'clock, middle third, lesion deeper and posterior to the surgical scar. Right supraclavicular and right axillary metastatic nodes |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 2.0 × 1.8 cm |
| • Shape: | Irregular |
| • Margins: | Indistinct |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | Vascular calcification in both breasts |
| • Suspicious: | Fine pleomorphic |
| • Distribution: | Grouped in the mass |
| ‣ Architectural distortion: | Postoperative scar |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Fine pleomorphic calcifications in the mass, enlarged metastatic right supraclavicular and right axillary lymph nodes, and skin thickening along the surgical scar |
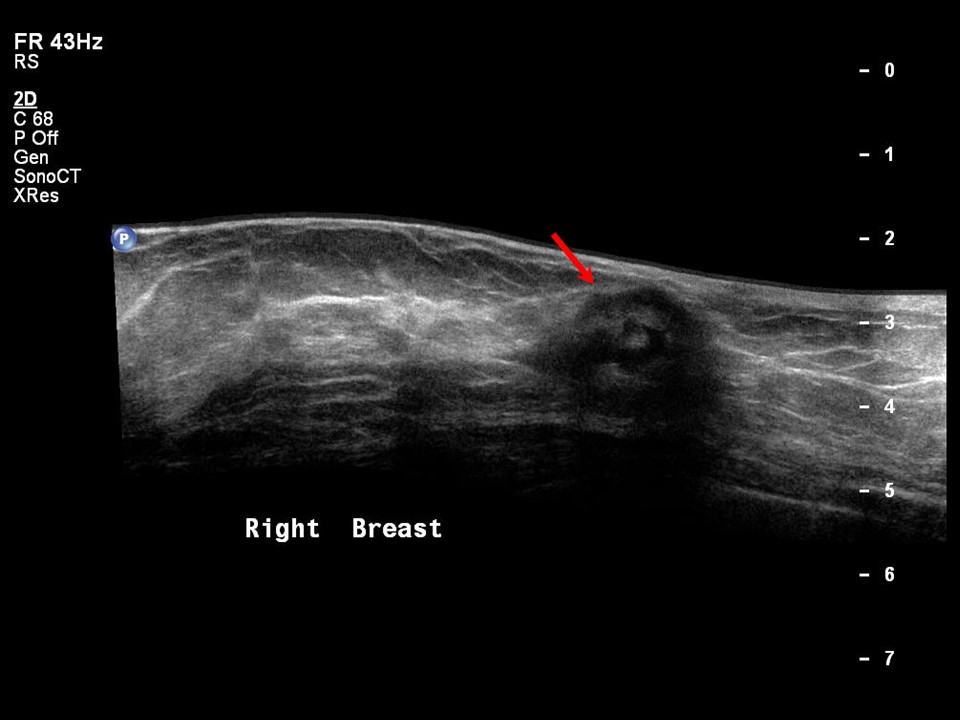
Ultrasound:
 | 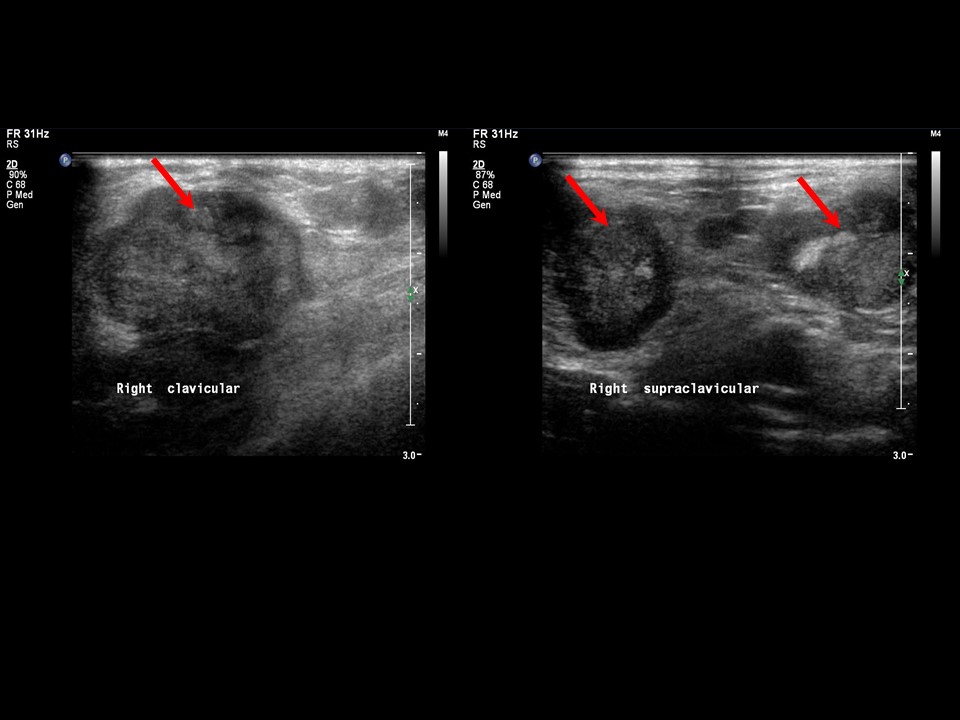 |
 | 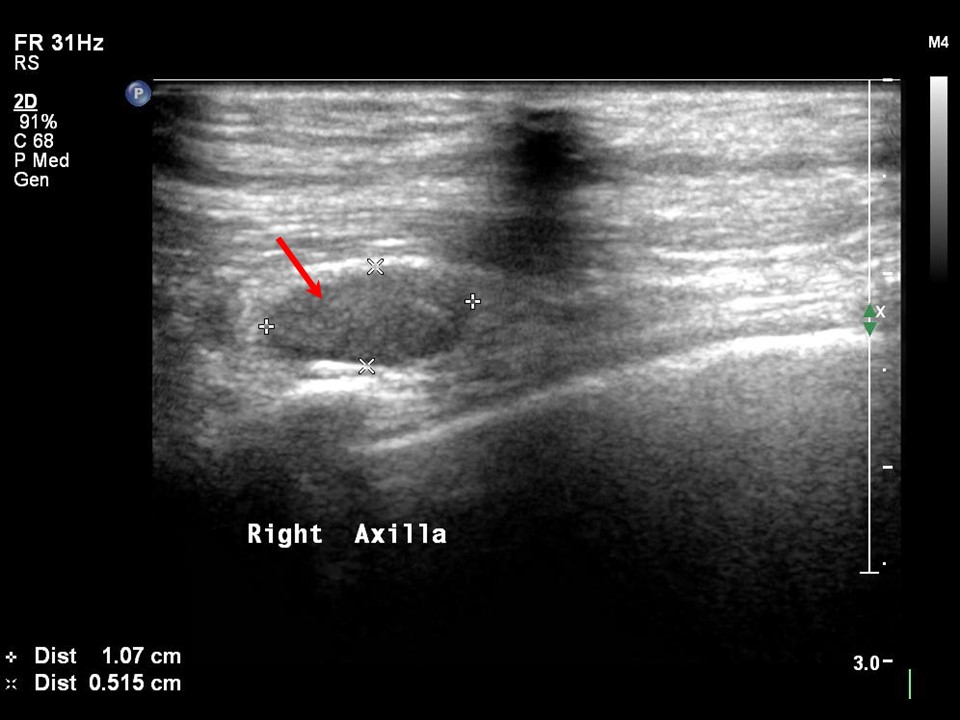 |
| Ultrasound features: Right breast, upper inner quadrant at 1 o'clock, deeper than and posterior to surgical scar from previous breast-conserving surgery | |
| ‣ Mass | |
| • Location: | Right breast, upper inner quadrant at 1 o'clock, deeper than and posterior to surgical scar from previous breast-conserving surgery |
| • Number: | 1 |
| • Size: | 2.0 × 1.8 cm |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Indistinct |
| • Echo pattern: | Heteroechoic with central anechoic component |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | Fine microcalcifications in mass |
| ‣ Associated features: | Skin thickening and right axillary and right supraclavicular metastatic lymphadenopathy |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category (Right BCS, post operative breast): 5 (highly suggestive of malignancy)Further assessment:
Further assessment advised: Referral for cytologyCytology:
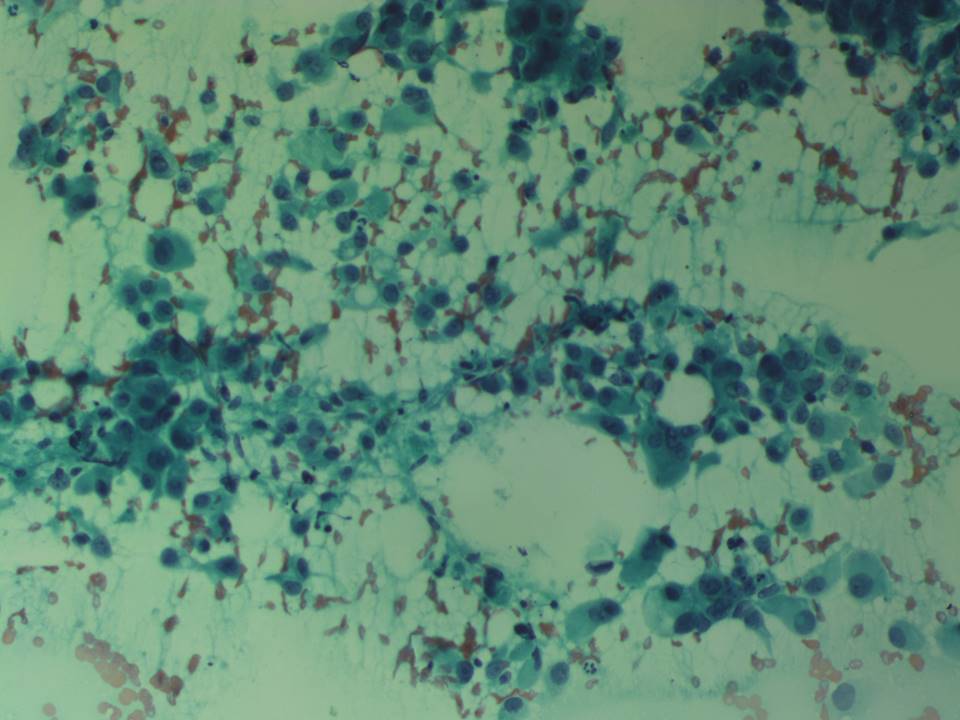 |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Right |
| • Quadrant: | Right supraclavicular lymph nodes |
| • Localization technique: | Palpation |
| • Nature of aspirate: | 0.3 mL of haemorrhagic aspirate |
| ‣ Cytological description: | Smears reveal mainly pleomorphic malignant cells with hyperchromatic nuclei and anisonucleosis with moderate cytoplasm. Mature lymphocytes are seen in the background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Metastases in right supraclavicular node |
| ‣ Comments: | None |
Case summary:
| Postmenopausal woman with increased risk of breast cancer presented with a right supraclavicular node first noticed 1 month ago with progressive increase in size since then. She underwent surgery for right breast cancer 6 years ago. On examination, a hard, non-tender right supraclavicular lump was palpable. A right breast surgical scar was seen with a palpable, diffuse, firm to hard area beneath the scar. Mammography and breast ultrasound revealed an irregular suspicious lesion with pleomorphic microcalcifications in the right breast and right axillary and supraclavicular enlarged nodes of altered morphology suggestive of metastatic nodes. Diagnosed as highly suggestive of malignancy, BI-RADS 5 on imaging and as metastases in right supraclavicular node on cytology. |
Learning points:
|